

Knee
Normal Anatomy of The Knee Joint
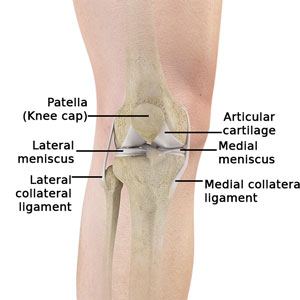
The knee is made up of four bones. The femur or thighbone is the bone connecting the hip to the knee. The tibia or shinbone connects the knee to the ankle. The patella (kneecap) is the small bone in front of the knee and rides on the knee joint as the knee bends. The fibula is a shorter and thinner bone running parallel to the tibia on its outside. The joint acts like a hinge but with some rotation.
The knee is a synovial joint, which means it is lined by synovium. The synovium produces fluid lubricating and nourishing the inside of the joint. Articular cartilage is the smooth surfaces at the end of the femur and tibia. It is the damage to this surface which causes arthritis.
Femur
The femur (thighbone) is the largest and the strongest bone in the body. It is the weight bearing bone of the thigh. It provides attachment to most of the muscles of the knee.
Condyle
The two femoral condyles make up for the rounded end of the femur. Its smooth articular surface allows the femur to move easily over the tibial (shinbone) meniscus.
Tibia
The tibia (shinbone), the second largest bone in the body, is the weight bearing bone of the leg. The menisci incompletely cover the superior surface of the tibia where it articulates with the femur. The menisci act as shock absorbers, protecting the articular surface of the tibia as well as assisting in rotation of the knee.
Fibula
The fibula, although not a weight bearing bone, provides attachment sites for the Lateral collateral ligaments (LCL) and the biceps femoris tendon.
The articulation of the tibia and fibula also allows a slight degree of movement, providing an element of flexibility in response to the actions of muscles attaching to the fibula.
Patella
The patella (kneecap), attached to the quadriceps tendon above and the patellar ligament below, rests against the anterior articular surface of the lower end of the femur and protects the knee joint. The patella acts as a fulcrum for the quadriceps by holding the quadriceps tendon off the lower end of the femur.
Menisci
The medial and the lateral meniscus are thin C-shaped layers of fibrocartilage, incompletely covering the surface of the tibia where it articulates with the femur. The majority of the meniscus has no blood supply and for that reason, when damaged, the meniscus is unable to undergo the normal healing process that occurs in the rest of the body. The menisci act as shock absorbers, protecting the articular surface of the tibia as well as assisting in rotation of the knee. As secondary stabilizers, the intact menisci interact with the stabilizing function of the ligaments and are most effective when the surrounding ligaments are intact.
Anterior Cruciate Ligament (ACL)
The anterior cruciate ligament (ACL) is the major stabilizing ligament of the knee. The ACL is located in the center of the knee joint and runs from the femur (thigh bone) to the tibia (shin bone), through the center of the knee. The ACL prevents the femur from sliding backwards on the tibia (or the tibia sliding forwards on the femur). Together with the posterior cruciate ligament (PCL), ACL stabilizes the knee in a rotational fashion. Thus, if one of these ligaments is significantly damaged, the knee will be unstable when planting the foot of the injured extremity and pivoting, causing the knee to buckle and give way.
Posterior Cruciate Ligament (PCL)
Much less research has been done on the posterior cruciate ligament (PCL) because it is injured far less often than the ACL.
The PCL prevents the femur from moving too far forward over the tibia. The PCL is the knee's basic stabilizer and is almost twice as strong as the ACL. It provides a central axis about which the knee rotates.
Collateral Ligaments
Collateral Ligaments prevent hyperextension, adduction, and abduction
- Superficial MCL (Medial Collateral Ligament) connects the medial epicondyle of the femur to the medial condyle of the tibia and resists valgus force
- Deep MCL (Medial Collateral Ligament) connects the medial epicondyle of the femur with the medial meniscus
- LCL (Lateral Collateral Ligament) entirely separate from the articular capsule, connects the lateral epicondyle of the femur to the head of the fibula and resists varus force
Arthroscopy Of The Knee Joint
Knee Arthroscopy is a common surgical procedure performed using an arthroscope, a viewing instrument, to look into the knee joint to diagnose or treat a knee problem. It is a relatively safe procedure and a majority of the patient's discharge from the hospital on the same day of surgery.
Knee anatomy
The knee joint is one of the most complex joints of the body. The lower end of the thighbone (femur) meets the upper end of the shinbone (tibia) at the knee joint. A small bone called the patella (kneecap) rests on a groove on the front side of the femoral end. A bone of the lower leg (fibula) forms a joint with the shinbone.
To allow smooth and painless motion of the knee joint, articular surfaces of these bones are covered with a shiny white slippery articular cartilage. Two C-shaped cartilaginous menisci are present in between the femoral end and the tibial end.
Menisci act as shock absorbers providing cushion to the joints. Menisci also play an important role in providing stability and load bearing to the knee joint.
Bands of tissue, including the cruciate and collateral ligaments, keep the different bones of the knee joint together and provide stabilization to the joint. Surrounding muscles are connected to the knee bones by tendons. The bones work together with the muscles and tendons to provide mobility to the knee joint. The whole knee joint is covered by a ligamentous capsule, which further stabilizes the joint. This ligamentous capsule is also lined with a synovial membrane that secretes synovial fluid for lubrication.
Indications for Knee arthroscopy
The knee joint is vulnerable to a variety of injuries. The most common knee problems where knee arthroscopy may be recommended for diagnosis and treatment are:
- Torn meniscus
- Torn or damaged cruciate ligament
- Torn pieces of articular cartilage
- Inflamed synovial tissue
- Misalignment of patella
- Baker's cyst: a fluid filled cyst that develops at the back of the knee due to the accumulation of synovial fluid. It commonly occurs with knee conditions such as meniscal tear, knee arthritis and rheumatoid arthritis.
- Certain fractures of the knee bones
Procedure
Knee arthroscopy is performed under local, spinal, or general anesthesia. Your anesthesiologist will decide the best method for you depending on your age and health condition.
- The surgeon makes two or three small incisions around the knee.
- Next, a sterile saline solution is injected into the knee to push apart the various internal structures. This provides a clear view and more room for the surgeon to work.
- An arthroscope, a narrow tube with a tiny video camera on the end, is inserted through one of the incisions to view the knee joint. The structures inside the knee are visible to the surgeon on a video monitor in the operating room.
- The surgeon first examines the structures inside the knee joint to assess the cause of the problem.
- Once a diagnosis is made, surgical instruments such as scissors, motorized shavers, or lasers are inserted through another small incision, and the repair is performed based on the diagnosis.
The repair procedure may include any of the following:
- Removal or repair of a torn meniscus
- Reconstruction or repair of a torn cruciate ligament
- Removal of small torn pieces of articular cartilage
- Removal of loose fragments of bones
- Removal of inflamed synovial tissue
- Removal of baker's cyst
- Realignment of the patella
- Making small holes or microfractures near the damaged cartilage to stimulate cartilage growth
- After the repair, the knee joint is carefully examined for bleeding or any other damage.
- The saline is then drained from the knee joint.
- Finally, the incisions are closed with sutures or steri-strips, and the knee is covered with a sterile dressing.
After the Surgery
Most patients are discharged the same day after knee arthroscopy. Recovery after the surgery depends on the type of repair procedure performed. Recovery from simple procedures is often fast. However, recovery from complicated procedures takes a little longer. Recovery from knee arthroscopy is much faster than that from an open knee surgery.
Pain medicines are prescribed to manage pain. Crutches or a knee brace may be recommended for several weeks. A rehabilitation program may also be advised for a successful recovery. Therapeutic exercises aim to restore motion and strengthen the muscles of the leg and knee.
Risks and complications
Knee arthroscopy is a safe procedure and complications are very rare. Complications specific to knee arthroscopy include bleeding into the knee joint, infection, knee stiffness, blood clots or continuing knee problems.
ACL Tear & Reconstruction
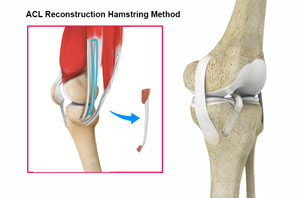
Anterior cruciate ligament (ACL) reconstruction hamstring method is a surgical procedure that replaces the injured ACL with a hamstring tendon. Anterior cruciate ligament is one of the four major ligaments of the knee that connects the femur (thigh bone) to the tibia (shin bone) and helps stabilize your knee joint. Anterior cruciate ligament prevents excessive forward movement of the lower leg bone (the tibia) in relation to the thigh bone (the femur) as well as limits rotational movements of the knee.
A tear of this ligament can make you feel as though your knees will not allow you to move or even hold you up. Anterior cruciate ligament reconstruction is surgery to reconstruct the torn ligament of your knee with a tissue graft.
Causes
An ACL injury most commonly occurs during sports that involve twisting or overextending your knee. An ACL can be injured in several ways:
- Sudden directional change
- Slowing down while running
- Landing from a jump incorrectly
- Direct blow to the side of your knee, such as during a football tackle
Symptoms
When you injure your ACL, you might hear a loud "pop" sound and you may feel the knee buckle. Within a few hours after an ACL injury, your knee may swell due to bleeding from vessels within the torn ligament. You may notice that the knee feels unstable or seems to give way, especially when trying to change direction on the knee.
Diagnosis
An ACL injury can be diagnosed with a thorough physical examination of the knee and diagnostic tests such as X-rays, MRI scans and arthroscopy. X-rays may be needed to rule out any fractures. In addition, your doctor will often perform the Lachman's test to see if the ACL is intact. During a Lachman test, knees with a torn ACL may show increased forward movement of the tibia and a soft or mushy endpoint compared to a healthy knee.
Pivot shift test is another test to assess ACL tear. During this test, if the ACL is torn, the tibia will move forward when the knee is completely straight and as the knee bends past 30° the tibia shifts back into correct place in relation to the femur.
Procedure
The goal of ACL reconstruction surgery is to tighten your knee and to restore its stability.
Anterior cruciate ligament reconstruction hamstring method is a surgical procedure to replace the torn ACL with part of the hamstring tendon taken from the patient's leg. The Hamstring is the muscle located on the back of your thigh. The procedure is performed under general anesthesia. Your surgeon will make two small cuts about 1/4 inch long around your knee. An arthroscope, a tube with a small video camera on the end is inserted through one incision to see the inside of the knee joint. Along with the arthroscope, a sterile solution is pumped into the joint to expand it enabling the surgeon to have a clear view and space to work inside the joint. The knee is bent at right angles and the hamstring tendons felt. A small incision is made over the hamstring tendon attachment to the tibia and the two tendons are stripped off the muscle and the graft is prepared. The torn ACL will be removed and the pathway for the new ACL is prepared. The arthroscope is reinserted into the knee joint through one of the small incisions. Small holes are drilled into the upper and lower leg bones where these bones come together at the knee joint. The holes form tunnels in your bone to accept the new graft. Then the graft is pulled through the predrilled holes in the tibia and femur. The new tendon is then fixed into the bone with screws to hold it into place while the ligament heals into the bone. The incisions are then closed with sutures and a dressing is placed.
Risks and complications
Possible risks and complications associated with ACL reconstruction with hamstring method include:
- Numbness
- Infection
- Blood clots (Deep vein thrombosis)
- Nerve and blood vessel damage
- Failure of the graft
- Loosening of the graft
- Decreased range of motion
- Crepitus (crackling or grating feeling of the kneecap)
- Pain in the knee
- Repeat injury to the graft
Post-operative care
Following the surgery, rehabilitation begins immediately. A physical therapist will teach you specific exercises to be performed to strengthen your leg and restore knee movement. Avoid competitive sports for 5 to 6 months to allow the new graft to incorporate into the knee joint.
Anterior cruciate ligament reconstruction is a very common and successful procedure. It is usually indicated in patients wishing to return to an active lifestyle especially those wishing to play sports involving running and twisting. Anterior cruciate ligament injury is a common knee ligament injury. If you have injured your ACL, surgery may be needed to regain full function of your knee.
ACL Reconstruction Patellar Tendon
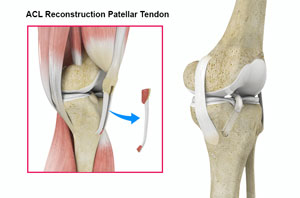
Anterior cruciate ligament (ACL) reconstruction patellar tendon is a surgical procedure that replaces the injured ACL with a patellar tendon. Anterior cruciate ligament is one of the four major ligaments of the knee that connects the femur (thigh bone) to the tibia (shin bone) and helps stabilize the knee joint. Anterior cruciate ligament prevents excessive forward movement of the lower leg bone (tibia) in relation to the thigh bone (femur) as well as limits rotational movements of the knee.
A tear of this ligament can make you feel as though your knees will not allow you to move or even hold you up. Anterior cruciate ligament reconstruction is surgery to reconstruct the torn ligament of your knee with a tissue graft.
Causes
An ACL injury most commonly occurs during sports that involve twisting or overextending your knee. The ACL can be injured in several ways:
- Sudden directional change
- Slowing down while running
- Landing from a jump incorrectly
- Direct blow to the side of your knee, such as during a football tackle
Symptoms
When you injure your ACL, you might hear a loud "pop" sound and you may feel the knee buckle. Within a few hours after an ACL injury, your knee may swell due to bleeding from vessels within the torn ligament. You may notice that the knee feels unstable or seems to give way, especially when trying to change direction on the knee.
Diagnosis
An ACL injury can be diagnosed with a thorough physical examination of the knee and diagnostic tests such as X-rays, MRI scans and arthroscopy. X-rays may be needed to rule out any fractures.
In addition, your doctor will often perform the Lachman's test to see if the ACL is intact. During a Lachman test, knees with a torn ACL may show increased forward movement of the tibia and a soft or mushy endpoint compared to a healthy knee.
Pivot shift test is another test to assess ACL tear. During the pivot shift test, if the ACL is torn the tibia will move forward when the knee is completely straight and as the knee bends past 30° the tibia shifts back into correct place in relation to the femur.
Procedure
The goal of ACL reconstruction surgery is to tighten your knee and to restore its stability.
Anterior cruciate ligament reconstruction patellar tendon is a surgical procedure to replace the torn ACL with part of the patellar tendon taken from the patient's leg. The new ACL is harvested from the patellar tendon that connects the bottom of the kneecap (patella) to the top of the shinbone (tibia). The procedure is performed under general anesthesia. Your surgeon will make two small cuts about ¼ inch around your knee. An arthroscope, a tube with a small video camera on the end is inserted through one incision to see the inside of the knee joint. Along with the arthroscope, a sterile solution is pumped into the knee to expand it providing the surgeon a clear view of the inside of the joint. The torn ACL will be removed and the pathway for the new ACL is prepared. Your surgeon makes an incision over the patellar tendon and takes out the middle third of the patellar tendon, along with small plugs of bone where it is attached on each end. The remaining portions of the patellar tendon on either side of the graft are sutured back after its removal. Then the incision is closed. The arthroscope is reinserted into the knee joint through one of the small incisions. Small holes are drilled into the upper and lower leg bones where these bones come together at the knee joint. The holes form tunnels in your bone to accept the new graft. Then the graft is pulled through the predrilled holes in the tibia and femur. The new tendon is then fixed into the bone with screws to hold it into place while the ligament heals into the bone. The incisions are then closed with sutures and a dressing is placed.
Risks and complications
Possible risks and complications associated with ACL reconstruction with patellar tendon method include:
- Numbness
- Infection
- Blood clots (Deep vein thrombosis)
- Nerve and blood vessel damage
- Failure of the graft
- Loosening of the graft
- Decreased range of motion
- Crepitus (crackling or grating feeling of the kneecap)
- Pain in the knee
- Repeat injury to the graft
Post-operative care
Following the surgery rehabilitation begins immediately. A physical therapist will teach you specific exercises to strengthen your leg and restore knee movement. Avoid competitive sports for 5 to 6 months to allow the new graft to incorporate into the knee joint.
Anterior cruciate ligament reconstruction is a very common and successful procedure. It is usually indicated in patients who desire to return to an active lifestyle especially those wishing to play sports involving running and twisting. Anterior cruciate ligament injury is a common knee ligament injury. If you have injured your anterior cruciate ligament, surgery may be needed to regain full function of your knee.
Meniscus Tear

Meniscus tear is the commonest knee injury in athletes, especially those involved in contact sports. A suddenly bend or twist in your knee cause the meniscus to tear. This is a traumatic meniscus tear. Elderly people are more prone to degenerative meniscal tears as the cartilage wears out and weakens with age. The two wedge-shape cartilage pieces present between the thighbone and the shinbone are called meniscus. They stabilize the knee joint and act as "shock absorbers".
Torn meniscus causes pain, swelling, stiffness, catching or locking sensation in your knee making you unable to move your knee through its complete range of motion. Your orthopedic surgeon will examine your knee, evaluate your symptoms, and medical history before suggesting a treatment plan. The treatment depends on the type, size and location of tear as well your age and activity level. If the tear is small with damage in only the outer edge of the meniscus, nonsurgical treatment may be sufficient. However, if the symptoms do not resolve with nonsurgical treatment, surgical treatment may be recommended.
Surgical Treatment
Knee arthroscopy is the commonly recommended surgical procedure for meniscal tears. The surgical treatment options include meniscus removal (meniscectomy), meniscus repair, and meniscus replacement. Surgery can be performed using arthroscopy where a tiny camera will be inserted through a tiny incision which enables the surgeon to view inside of your knee on a large screen and through other tiny incisions, surgery will be performed. During meniscectomy, small instruments called shavers or scissors may be used to remove the torn meniscus. In arthroscopic meniscus repair the torn meniscus will be pinned or sutured depending on the extent of tear.
Meniscus replacement or transplantation involves replacement of a torn cartilage with the cartilage obtained from a donor or a cultured patch obtained from laboratory. It is considered as a treatment option to relieve knee pain in patients who have undergone meniscectomy.
Multi-Ligament Injury
Multi-ligament injury in Adults
Ligaments are the fibrous tissue brands connecting the bones in the joint and stabilizing the joint. Knee joint has 2 sets of ligaments-collateral ligaments (medial and collateral ligaments) that connect the bones on outer side of the knee and cruciate ligaments (anterior cruciate ligament and posterior cruciate ligament) those present inside the joint. Multi-ligament injury is the injury to multiple ligaments at the same time. Damage to three or more ligaments may cause joint dislocation.
Multi-ligament injuries occur as a result of major trauma such as a direct blow to the knee, or a fall from a height, or motor vehicle trauma.
Patients with multi-ligament knee injuries may experience pain, swelling, limited range of motion, injuries to nerves and arteries of the leg, and knee instability.
Most multi-ligament knee injuries require surgery to reconstruct ligaments. This serious and complex injury may require more than one surgical procedure to stabilize the knee. Ligaments are reconstructed using a graft taken from the patient, or frequently donor tissue to create a new ligament. Surgical reconstruction is usually performed using arthroscope, during which tunnels are created in the thigh and tibia bone using a small drill to allow the grafts to be placed into the knee and to replace the torn ligaments. After the grafts are placed, screws, washers, and other fixation devices are used to secure the grafts in place and to help hold the ligament in place until healing takes place. After multiligament knee reconstruction, crutches may be required for 6 to 8 weeks.
Following multiligament knee reconstruction, the most common complications include recurrent instability, stiffness, loss of motion, scar tissue formation, and injury to nerves and blood vessels.
Multi-ligament injury in Children
The skeletally immature knee slightly differs from the adult knee and may result in mild variations of injury patterns. In children, the epiphyseal plates (growth plates or physis) are weak compared with ligaments in the adults. Growth plate is the area of growing tissue made up of cartilage found at the ends of the long bones in children. Therefore, any extraneous force on the knee causes physeal injury rather than the ligament injury.
Growth plate injuries commonly occur in growing children and teenagers. Traditionally most multi-ligament knee injuries require surgery to reconstruct ligaments that involves drilling holes in the bone through the area of the growth plate. In a skeletally immature child the growth plates are open. Therefore, other treatment options, especially physeal-sparing surgery, a reconstruction procedure that avoids drilling holes through the growth plate may be done.
You may need to discuss with your doctor about what treatment options and how to make a decision that you and your child will be comfortable with.
PCL Tear & Reconstruction
Posterior cruciate ligament (PCL), one of four major ligaments of the knee is situated at the back of the knee. It connects the thighbone (femur) to the shinbone (tibia). The PCL limits the backward motion of the shinbone.
PCL injuries are very rare and are difficult to detect than other knee ligament injuries. Cartilage injuries, bone bruises, and ligament injuries often occur in combination with PCL injuries. Injuries to the PCL can be graded as I, II or III depending on the severity of injury. In grade I the ligament is mildly damaged and slightly stretched, but the knee joint is stable. In grade II there is partial tear of the ligament. In grade III there is complete tear of the ligament and the ligament is divided into two halves making the knee joint unstable.
The PCL is usually injured by a direct impact, such as in an automobile accident when the bent knee forcefully strikes the dashboard. In sports, it can occur when an athlete falls to the ground with a bent knee. Twisting injury or overextending the knee can cause the PCL to tear.
Patients with PCL injuries usually experience knee pain and swelling immediately after the injury. There may also be instability in the knee joint, knee stiffness that causes limping, and difficulty in walking.
Diagnosis of a PCL tear is made on the basis of your symptoms, medical history, and by performing a physical examination of the knee. Other diagnostic tests such as X-rays and MRI scan may be ordered. X-rays are useful to rule out avulsion fractures wherein the PCL tears off a piece of bone along with it. An MRI scan is done to help view the images of soft tissues better.
Treatment options may include non-surgical and surgical treatment. Non-surgical treatment consists of rest, ice, compression, and elevation (RICE protocol); all assist in controlling pain and swelling. Physical therapy may be recommended to improve knee motion and strength. A knee brace may be needed to help immobilize your knee. Crutches may be recommended to protect your knee and avoid bearing weight on your leg.
Generally, surgery is considered in patients with dislocated knee and several torn ligaments including the PCL. Surgery involves reconstructing the torn ligament using a tissue graft which is taken from another part of your body, or a cadaver (another human donor). Surgery is usually carried out with an arthroscope using small incisions. The major advantages of this technique include minimal postoperative pain, short hospital stay, and a fast recovery. Following PCL reconstruction, a rehabilitation program will be started that helps you resume a wider range of activities. Usually, a complete recovery may take about 6 to 12 months.
MCL Sprain
The medial collateral ligament (MCL), a band of tissue present on the inside of your knee joint, connects your thigh bone and shin bone (bone of your lower leg). The MCL maintains the integrity of the knee joint and prevents it from bending inward.
Your MCL may get sprained or injured while twisting, bending or quickly changing direction. The sprain is classified into three degrees:
- First-degree sprain: Ligament fibers may be injured, but with no significant tear and no loss of integrity
- Second-degree sprain: Not all ligament fibers are torn. Ligament remains intact overall
- Third-degree sprain: Complete rupture of ligament and loss of overall integrity
Causes
MCL sprains occur due to sudden impact from the outside of your knee, most commonly while playing sports such as rugby and football. Rarely, the MCL can get injured when the knee gets twisted or following a quick change in direction.
Symptoms
The symptoms of MCL sprain include:
- Tenderness and pain in the inner side of the knee
- Swelling and bruising
- Stiffness of knee
- Difficulty walking
- Bleeding and inflow of fluid into the joint
Diagnosis
Your doctor will review your symptoms and medical history. Physical examination will be performed where your doctor checks the range-of-movement of your legs. An X-ray or MRI scan may be ordered to determine soft tissue injury, confirm the extent of damage, and assess the integrity of your knee.
Treatment
MCL sprains are commonly treated by conservative procedures. You will be advised to take adequate rest and not to strain yourself. An ice pack may be applied for 10 to 20 minutes for every 1 to 2 hours to reduce swelling. You may be prescribed anti-inflammatory medicines to reduce the pain and swelling. Your doctor may recommend crutches and braces to support, protect and limit movement in your knee. Rehabilitation procedures and exercises for MCL sprains generally focus on regaining knee range-of-motion, muscle control and strength, and reduce swelling. Surgery is performed very rarely, in case of significant third-degree ligament injury.
Based on your extent of damage, your doctor will suggest the best possible treatment option to treat your MCL sprain.
Patellofemoral Dislocation
Patella (knee cap) is a protective bone attached to the quadriceps muscles of the thigh by quadriceps tendon. Patella attaches with the femur bone and forms a patellofemoral joint. Patella is protected by a ligament which secures the kneecap from gliding out and is called as medial patellofemoral ligament (MPFL).
Dislocation of the patella occurs when the patella moves out of the patellofemoral groove, (called as trochlea) onto a bony head of the femur. If the knee cap partially comes out of the groove, it is called as subluxation and if the kneecap completely comes out, it is called as dislocation (luxation). Patella dislocation is commonly observed in young athletes between 15 and 20 years and commonly affects women because of the wider pelvis creates lateral pull on the patella.
Some of the causes for patellar dislocation include direct blow or trauma, twisting of the knee while changing the direction, muscle contraction, and congenital defects. It also occurs when the MPFL is torn. The common symptoms include pain, tenderness, swelling around the knee joint, restricted movement of the knee, numbness below the knee, and discoloration of the area where the injury has occurred.
Your doctor will examine your knee and suggests diagnostic tests such as X-ray, CT scan, and MRI scan to confirm condition and provide treatment. There are non-surgical and surgical ways of treating patellofemoral dislocation.
Non-surgical or conservative treatment includes:
- PRICE (protection, rest, ice, compression, and elevation)
- Nonsteroidal anti-inflammatory drugs and analgesics to treat pain and swelling
- Braces or casts which will immobilize the knee and allows the MPF ligament to heal
- Footwear to control gait while walking or running and also decreases the pressure on the kneecap.
- Physical therapy is recommended which helps to control pain and swelling, prevent formation of scar of soft tissue, and also helps in collagen formation. Physiotherapist will extend your knee and applies direct lateral to medial pressure to the knee which helps in relocation. It includes straightening and strengthening exercises of the hip muscles and other exercises which will improve range of motion.
Surgical treatment is recommended for those individuals who have recurrent patella dislocation. Some of the surgical options include:
- Lateral-release- It is done to loosen or release the tight lateral ligaments that pull the kneecap from its groove which increases pressure on the cartilage and causes dislocation. In this procedure, the ligaments that tightly hold the kneecap are cut using an arthroscope.
- Medial patellofemoral ligament reconstruction- In this procedure, the torn MPF ligament is removed and reconstructed using grafting technique. Grafts are usually harvested from the hamstring tendons, located at the back of the knee and are fixed to the patella tendon using screws. The grafts are either taken from the same individuals (autograft) or from a donor (allograft). This procedure is also performed using an arthroscope.
- Tibia tubercle realignment or transfer- Tibia tubercle is a bony attachment below the patella tendon which sits on the tibia. In this procedure, the tibia tubercle is moved towards the center which is then held by two screws. The screws hold the bone in place and allow faster healing and prevent the patella to slide out of the groove. This procedure is also performed using an arthroscope.
After the surgery, your doctor will suggest you to use crutches for few weeks, prescribe medications to control pain and swelling, and recommend physical therapy which will help you to return to your sports activities at the earliest.
Patellofemoral Pain
Patellofemoral pain syndrome also called runner's knee refers to pain under and around your kneecap. Patellofemoral pain is seen in number of medical conditions such as anterior knee pain syndrome, patellofemoral malalignment, and chondromalacia patella that cause pain around the front of the knee. Patellofemoral pain is a common complaint among runners, jumpers, and other athletes such as skiers, cyclists, and soccer players and therefore is the common name, runner's knee.
Causes
Patellofemoral pain can result from poor alignment of the kneecap, complete or partial dislocation, overuse, tight or weak thigh muscles, flat feet, direct trauma to the knee. Patellofemoral pain often comes from strained tendons and irritation or softening of the cartilage that lines the underside of the kneecap. Pain in the knee may be referred from other parts of the body, such as the back or hip.
Symptoms
The most common symptom includes a dull aching pain underneath the kneecap while walking up or down stairs, squatting, kneeling down, and sitting with your knees bent for long period of time.
Pain usually occurs under or around the front of the kneecap (patella) where it attaches with the lower end of the thighbone (femur). The patella, also called kneecap, is a small flat triangular bone located at the front of the knee joint. The kneecap or patella is a sesamoid bone that is embedded in a tendon that connects the muscles of the thigh to the shin bone (tibia). The function of the patella is to protect the front part of the knee.
Diagnosis
To diagnose patellofemoral pain, your doctor will ask about your symptoms, medical history, any sports participation, and activities that aggravate your knee pain. Your doctor will perform a physical examination of your knee. Diagnostic imaging tests such as X-rays, MRIs, and CT scans, and blood tests may be ordered to check if your pain is due to damage to the structure of the knee or because of the tissues that attach to it.
Treatment
The first treatment step is to avoid activities such as running and jumping, that causes pain. Treatment options include both non-surgical and surgical methods. Non-surgical treatment consists of rest, ice, compression, and elevation (RICE protocol); all assist in controlling pain and swelling. Non-steroidal anti-inflammatory medications may be prescribed to reduce pain.
Exercises: Your doctor may recommend exercise program to improve the flexibility and strength of thigh muscles. Cross-training exercises to stretch the lower extremities may also be recommended by your doctor.
Other non-surgical treatments include:
- Knee taping: An adhesive tape is applied over the patella, to alter the kneecap alignment and movement. Taping of the patella may reduce pain.
- Knee brace: A special brace for knee may be used during sports participation which may help reduce pain.
- Orthotics: Special shoe inserts may be prescribed for those with flat feet that may help relieve the pain.
In some cases, you may need surgery that includes arthroscopy and realignment. During arthroscopy, damaged fragments are removed from the kneecap, while realignment moves the kneecap back to its alignment, thus reducing the abnormal pressure on cartilage and supporting structures around the front of the knee.
Prevention
- If you are overweight, you may need to control your weight to avoid overstressing your knees
- Gradually increase the intensity of your workout
- If you have flat feet or other foot problems use shoe inserts
- Avoid running on hard surfaces
- Wear proper fitting good quality running shoes with good shock absorption
- Avoid running straight down hills; instead walk down it or run in a zigzag pattern
- Warm up for 5 minutes before starting any exercise. Also stretch after exercising
Chondromalacia/OCD
The patella, also called the kneecap, is a small bone present on the front of your knee joint. The underside of the patella is covered by cartilage that allows smooth gliding of the knee with movement. Overuse or misalignment of the patella can cause wear and tear of the cartilage.
Chondromalacia patella is a common condition characterized by softening, weakening and damage of the cartilage. The condition is most often seen among young athletes and older adults who have arthritis of the knee. It is especially seen in women.
Causes
There is no explicit reason why the cartilage damage occurs. However, it is associated with improper knee alignment or imbalance in the tightness of the muscles holding it in place. Overuse of the knee in certain sports activities may cause wear and tear of the cartilage. This may cause rubbing or grinding of the kneecap against the bone instead of it smoothly gliding over the knee joint.
Chondromalacia patella may also be caused due to injuries such as fractures or dislocations, or may develop as a part of your ageing process.
Symptoms
Chondromalacia patella is the most common cause of knee pain. Called patellofemoral pain, it is characterized by the following:
Pain in front, around or behind your knee
Pain that gets worse when climbing up or down the stairs, sitting or standing for long periods, or when extreme pressure is applied on the knee
Other symptoms may include:
- Grinding or cracking sensation or noise when you move your knee
- Occasionally, swelling or fluid effusion in your knee joint
Diagnosis
Your doctor will conduct a physical examination by applying pressure on different areas of your knee and moving your leg in different positions. You may be asked to undergo imaging tests including an X-ray, CT scan and MRI scan to obtain detailed images of the bones and soft tissues of the knee.
Treatment
The treatment of chondromalacia patella initially involves simple conservative procedures. You may be asked to rest your knee and avoid any activity that may strain the knee joint. Your doctor may prescribe painkillers and anti-inflammatory drugs to relieve pain and reduce swelling. Physiotherapy may help you to improve the muscle strength, decrease stress on your knee and aid in correcting the misalignment. Wearing support braces and taping around the knee may help you protect your joint, reduce pain and improve alignment. Application of ice on the knee may be recommended after exercise.
When non-surgical treatment does not relieve pain, your doctor may recommend surgical treatment. Surgery may involve:
Arthroscopy: your doctor inserts a device called an arthroscope (thin tube with a camera and light attached) through a small incision. This helps to clearly view the surgical site while other instruments are inserted to remove fragments of the damaged cartilage.
Realignment: your surgeon may operate on your knee to realign the position of your knee cap and release the pressure over the cartilage.
Your doctor will examine your condition and provide you with the best treatment option.
Articular Cartilage Disorders & OCD Lesions
Articular Cartilage Disorders
Articular or hyaline cartilage is the tissue lining the surface of the two bones in the knee joint. Cartilage helps the bones move smoothly against each other and can withstand the weight of the body during activities such as running and jumping. Articular cartilage does not have a direct blood supply to it so has less capacity to repair itself. Once the cartilage is torn it will not heal easily and can lead to degeneration of the articular surface, leading to development of osteoarthritis.
The damage in articular cartilage can affect people of all ages. It can be damaged by trauma such as accidents, mechanical injury such as a fall, or from degenerative joint disease (osteoarthritis) occurring in older people.
Patients with articular cartilage damage experience symptoms such as joint pain, swelling, stiffness, and a decrease in range of motion of the knee. Damaged cartilage needs to be replaced with healthy cartilage and the procedure is known as cartilage replacement. It is a surgical procedure performed to replace the worn-out cartilage and is usually performed to treat patients with small areas of cartilage damage usually caused by sports or traumatic injuries. It is not indicated for those patients who have advanced arthritis of knee.
Cartilage replacement helps relieve pain, restore normal function, and can delay or prevent the onset of arthritis. The goal of cartilage replacement procedures is to stimulate growth of new hyaline cartilage. Various arthroscopic procedures involved in cartilage replacement include:
- Microfracture
- Drilling
- Abrasion Arthroplasty
- Autologous chondrocyte implantation (ACI)
- Osteochondral Autograft Transplantation
OCD lesions
Osteochondritis dessicans is a condition of loosening or detachment of a fragment of cartilage and underlying a bone in a joint. The fragment may be localized, loosely float in the joint space, or completely detach from the cartilage or bone. Exact cause for osteochondritis dessicans remains unknown and certain factors such as trauma, fractures, sprains, or injury to the joint are considered to increase the risk of developing the condition. Following the injury or trauma, the bones in the area may be deprived of blood flow leading to necrosis and finally the bone fragment may break off. This may initiate the healing process however by this time, articular cartilage will be compressed, flattened, and a subchondral cyst will be developed. All these changes in addition to increased joint pressure cause failure of healing of the joint.
Patients with osteochondritis dessicans experience symptoms such as joint pain, stiffness, restricted motion of joints, and locking at the joint.
Your physician may recommend various treatments depending on the reports of diagnostic scans, age, severity, stability of the cartilage and other factors. Goals of treatment are to relieve the symptoms and stop or impede the progression of degeneration of the joint. Conservative treatment approaches such as wait & watch approach, pain medications, and immobilization for 1-2 weeks are recommended if the condition is diagnosed at early stages and if the severity is mild. However surgery is required if the condition is diagnosed at advanced stage or if the condition is severe.
The surgical correction of osteochondritis dessicans can be done using by open technique or arthroscopic techniques. Some of the surgical procedures include drilling, bone grafting, open reduction internal fixation, osteochondral grafting, or autologous chondrocyte implantation (ACI).
- Drilling – In this method multiple small holes are drilled into the bone which allows the growth of new blood vessels in the defect area. This promotes blood flow into defect area thereby initiating the healing response and formation of new cartilage cells inside the lesion.
- Open reduction internal fixation – Open surgery is performed in cases where the defected area is difficult to reach with arthroscope. Hence an open incision may be required. In this procedure an incision is made in front of the joint to allow the surgeon to see the joint and the loose bodies are removed. Internal fixation involves fixing the fragments using internal fixators such as metal screws, pins, or wires.
- Bone grafting – It helps to fill the gap after removal of the dead or necrotic bone. In this procedure bone graft is placed on the damaged site. This procedure may be performed to repair the damaged area or replace the missing bone. Autograft (harvested from the same individual) or allograft (taken from bone bank) may be required to help in the growth of a new bone.
- Osteochondral grafting - The procedure involves transfer of healthy cartilage plugs from the non-weight bearing areas of the joint and transferring into the damaged areas of the joint in mosaic pattern. It allows the newly implanted bone and cartilage to grow in the defected area. Grafts may be taken from the same individual (autograft) or from a donor or bone bank (allograft).
- Autologous chondrocyte implantation (ACI) – In this procedure healthy cartilage cells are harvested from the non weight-bearing joint of the patient and cultured in laboratory. The cultured cartilage tissue patch will be implanted into the defected area which also promotes the growth of new cartilage.
Knee Arthritis
Arthritis is a general term covering numerous conditions where the joint surface or cartilage wears out. The joint surface is covered by a smooth articular surface that allows pain free movement in the joint. This surface can wear out for a number of reasons; often the definite cause is not known.
When the articular cartilage wears out the bone ends rub on one another and cause pain. This condition is referred to as Osteoarthritis or “wear and tear” arthritis as it occurs with aging and use. It is the most common type of arthritis.
Causes of Arthritis
There are numerous conditions that can cause arthritis but often the exact cause is never known. In general, but not always, it affects people as they get older (Osteoarthritis). Other causes include:
- Trauma (fracture)
- Increased stress such as overuse and overweight
- Infection of the bone
- Connective tissue disorders
- Inactive lifestyle and Obesity (overweight); Your weight is the single most important link between diet and arthritis as being overweight puts an additional burden on your hips, knees, ankles and feet.
- Inflammation (Rheumatoid arthritis)
Symptoms
Knee Arthritis causes pain and decreased mobility of the knee joint. In the arthritic knee, there is an absent joint space that shows on X-ray. In the normal knee, there is a normal joint space.
Arthritic knee
The cartilage lining is thinner than normal or completely absent. The degree of cartilage damage and inflammation varies with the type and stage of arthritis. The capsule of the arthritic knee is swollen. The joint space is narrowed and irregular in outline; this can be seen in an X-ray image. Bone spurs or excessive bone can also build up around the edges of the joint. The combinations of these factors make the arthritic knee stiff and limit activities due to pain or fatigue.
Patella Fracture
The knee cap or patella is the largest sesamoid bone in the body and one of the components of the knee joint, present at the front of the knee. The undersurface of the kneecap and the lower end of the femur are coated with articular cartilage, which helps in smooth movement of the knee joint. The knee cap protects the knee and provides attachment to various muscle groups of the thigh and leg. Fracture of knee cap is rare and is more common in adult males.
Causes
The most common cause of fracture is a direct blow to the knee cap such as a fall or a motor vehicle accident. The patella can also be fractured indirectly, due to a sudden contraction of the thigh muscles.
Symptoms
Pain and swelling are the predominant symptoms of a patella fracture. A few patients may also experience inability to walk and difficulty in straightening the knee. Sometimes bruising may also be seen around the fracture site.
Diagnosis
The diagnosis of a patella fracture comprises of a physical examination, history of the injury and X-ray imaging to determine the nature and severity of the fracture. X-ray is the most common and widely used diagnostic tool for identification of fractures.
Treatment
The treatment of patellar fracture depends upon the severity and nature of the fracture.
Non-surgical treatment
Non-surgical treatment can be used when the patella has not been fragmented or displaced. Casts or splints may be used to straighten the knee and help in the healing process. Immobilization of the affected limb for 6 to 8 weeks may also be recommended.
Surgical treatment
Surgical treatment is needed if there is displacement of fractured fragments of the bone or the distance between the fractured parts is too far and would fail to heal. Immediate surgery is recommended in case of open fracture where the fractured site is exposed through the skin. The type of procedure to be conducted depends on the nature of the fracture. Transverse fractures are fixed with the help of wires and pins and a "figure-of-eight" configuration tension band while in a comminuted fracture, the small bone fragments are removed from the knee joint.
Surgical treatment is needed if there is displacement of fractured fragments of the bone or the distance between the fractured parts is too far and would fail to heal. Immediate surgery is recommended in case of open fracture where the fractured site is exposed through the skin. The type of procedure to be conducted depends on the nature of the fracture. Transverse fractures are fixed with the help of wires and pins and a "figure-of-eight" configuration tension band while in a comminuted fracture, the small bone fragments are removed from the knee joint.
Rehabilitation
Rehabilitation plays a vital role in helping patients resume their daily activities, after healing of the fracture. Treatment of the fracture may cause stiffness of the joint and weakness of the muscles. Physical therapy, joint mobilization and muscle strengthening exercises or weight bearing exercises are helpful in regaining strength and preventing deformities.