

Elbow
Normal Anatomy of The Elbow

The arm in the human body is made up of three bones that join together to form a hinge joint called the elbow. The upper arm bone or humerus connects from the shoulder to the elbow forming the top of the hinge joint. The lower arm or forearm consists of two bones, the radius and the ulna. These bones connect the wrist to the elbow forming the bottom portion of the hinge joint.
The elbow joint is actually three separate joints surrounded by a watertight sac called a joint capsule. This capsule surrounds the elbow joint and contains lubricating fluid called synovial fluid.
- Humerus
- Ulna
- Radius
The three joints of the elbow include:
- Ulnohumeral joint is where movement between the ulna and humerus occurs.
- Radiohumeral joint is where movement between the radius and humerus occurs.
- Proximal radioulnar joint is where movement between the radius and ulna occurs.
Our elbow is held in place and supported by various soft tissues.
- Cartilage
Shiny and smooth, cartilage allows smooth movement where two bones come in contact with each other. - Tendons
Tendons are soft tissue that connects muscles to bones to provide support. - Biceps Tendon
This tendon attaches the biceps muscle on the front of the arm to the radius allowing supination, rotation of the elbow. - Triceps Tendon
This tendon attaches the triceps muscle on the back of the arm to the ulna bone allowing the elbow to straighten. - Lateral Epicondyle
This bony prominence located just above the elbow on the outside is where the forearm muscles that straighten the fingers and wrist come together in one tendon to attach to the humerus. - Medial Epicondyle
This bony prominence located just above the elbow on the inside is where the muscles that bend the fingers and wrist come together in one tendon to attach to the humerus. - Ligaments
Ligaments are strong rope like tissue that connects bones to other bones and help hold tendons in place providing stability to joints. Ligaments around the elbow join to form a watertight sac called a joint capsule. This capsule surrounds the elbow joint and contains lubricating fluid called synovial fluid. - Medial collateral ligament
Located on the inside of the elbow this ligament connects the ulna to the humerus. - Lateral collateral ligament
Located on the outside of the elbow this ligament connects the radius to the humerus. - Annular ligament
This ligament forms a ring around the head of the radius bone, holding it tight against the ulna. - Quadrate ligament
This ligament also connects the radius to the ulna. - Muscles
Muscles are fibrous tissue capable of contracting to cause body movement. - Biceps
This is the large muscle on the front of the arm above the elbow that allows elbow supination, rotation of the elbow. - Triceps
This is the large muscle on the back of the arm above the elbow enabling elbow extension, straightening of the elbow. - Brachialis
This muscle is the primary elbow flexor enabling bending of the elbow. It is located at the distal end of the humerus. - Wrist extensors
These muscles of the forearm attach to the lateral epicondyle enabling extension of the hand and wrist. - Wrist flexors
These muscles of the forearm attach to the medial epicondyle enabling flexion of the hand and wrist. - Nerves
Nerves are responsible for carrying signals back and forth from the brain to muscles in our body, enabling movement and sensation such as touch, pain, and hot or cold. - Radial nerve
- Ulnar nerve
- Median nerve
- Blood Vessels
The main vessel of the arm is the brachial artery. This artery travels across the inside of the elbow at the bend and then splits into two branches below the elbow. - Bursae
Bursae are small fluid filled sacs that decrease friction between tendons and bone or skin. Bursae contain special cells called synovial cells that secrete a lubricating fluid. When this fluid becomes infected, a common painful condition known as Bursitis can develop.
There are four main ligaments in the elbow.
The three main nerves of the arm are:
All three nerves begin at the shoulder and travel down the arm across the elbow.
These branches are:
Radial Artery: The radial artery is the largest artery supplying the hand and wrist area. Traveling across the front of the wrist, nearest the thumb, it is this artery that is palpated when a pulse is counted at the wrist.
Ulnar Artery: The ulnar artery travels next to the ulnar nerve through Guyon's canal in the wrist. It supplies blood flow to the front of the hand, fingers and thumb.
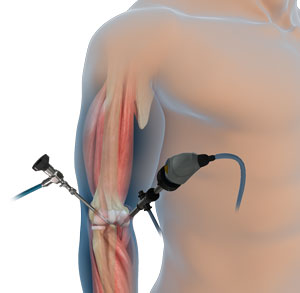
Elbow Arthroscopy
Elbow arthroscopy, also referred to as keyhole or minimally invasive surgery, is performed through tiny incisions to evaluate and treat several elbow conditions.
The Elbow is a complex hinge joint formed by the articulation of three bones - humerus, radius and ulna. The upper arm bone or humerus connects the shoulder to the elbow forming the upper portion of the hinge joint. The lower arm consists of two bones, the radius and the ulna. These bones connect the wrist to the elbow forming the lower portion of the hinge joint.
The three joints of the elbow are
- Ulnohumeral joint, the junction between the ulna and humerus
- Radiohumeral joint, the junction between the radius and humerus
- Proximal radioulnar joint, the junction between the radius and ulna
The elbow is held in place with the support of various soft tissues including:
- Cartilage
- Tendons
- Ligaments
- Muscles
- Nerves
- Blood vessels and
- Bursae
Indications of elbow arthroscopy:
Elbow arthroscopy is usually recommended for the following reasons:
- Debridement of loose bodies such as bone chips or torn cartilage tissue
- Removal of scar tissue
- Removal of bone spurs: These are extra bony growths caused by injury or arthritis that damage the ends of bones causing pain and limited mobility.
Arthroscopy is also used for the:
- Treatment of osteoarthritis, rheumatoid arthritis, and a condition called osteochondritis dissecans where loose fragments of cartilage and bone are in the joint space.
Evaluation and Diagnosis:
Your surgeon will review your medical history and perform a complete physical examination. Diagnostic studies may also be ordered such as X-rays, MRI or CT scan to assist in diagnosis.
Surgical Procedure
Arthroscopy is a surgical procedure in which an arthroscope, a small soft flexible tube with a light and video camera at the end, is inserted into a joint to evaluate and treat a variety of conditions.
Elbow arthroscopy is commonly performed under general anesthesia as an outpatient procedure. The patient is placed in a lateral or prone position which allows the surgeon to easily adjust the arthroscope and have a clear view of the inside of the elbow.
Several tiny incisions are made to insert the arthroscope and small surgical instruments into the joint. To enhance the clarity of the elbow structures through the arthroscope, your surgeon will fill the elbow joint with a sterile liquid.
The liquid flows through the arthroscope to maintain clarity and also to restrict any bleeding. The camera attached to the arthroscope displays the internal structures of the elbow on the monitor and helps your surgeon to evaluate the joint and direct the surgical instruments to fix the problem.
At the end of the procedure, the surgical incisions are closed by sutures, and a soft sterile dressing is applied. Your surgeon will place a cast or a splint to restrict the movement of the elbow.
The advantages of arthroscopy compared to traditional open elbow surgery include:
- Smaller incisions
- Minimal soft tissue trauma
- Less post-operative pain
- Faster healing time
- Lower infection rate
Post-operative care:
The post-surgical instructions include:
- Make sure to get adequate rest.
- Raise your elbow on pillows above the level of the heart to help reduce swelling.
- Keep the incision area clean and dry.
- A compressive stocking may be applied from the armpit to the hand once the dressing is removed to decrease pain and increase range of motion.
- Your doctor will prescribe pain medications to keep you comfortable.
- Physical therapy will be ordered to restore normal elbow strength.
- Eating a healthy diet and not smoking will promote healing.
Complications:
The possible complications following elbow arthroscopy include infection, bleeding, and damage to nerves or blood vessels.
Tennis Elbow(Lateral Epicondylitis)
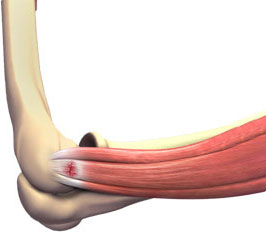
Tennis elbow is the common name used for the elbow condition called lateral epicondylitis. It is an overuse injury that causes inflammation of the tendons that attach to the bony prominence on the outside of the elbow (lateral epicondyle). It is a painful condition occurring from repeated muscle contractions at the forearm that leads to inflammation and micro tears in the tendons that attach to the lateral epicondyle. The condition is more common in sports activities such as tennis, painting, hammering, typing, gardening and playing musical instruments. Patients with tennis elbow experience elbow pain or burning that gradually worsens and results in a weakened grip.
Your doctor will evaluate tennis elbow by reviewing your medical history, performing a thorough physical examination and ordering X-rays, MRI or electromyogram (EMG) to detect any nerve compression.
Your doctor will first recommend conservative treatment options to treat the tennis elbow symptoms. These may include:
- Limit use and rest the arm from activities that worsen symptoms.
- Splints or braces may be ordered to decrease stress on the injured tissues.
- Apply ice packs on the elbow to reduce swelling.
- Avoid activities that bring on the symptoms and increase stress on the tendons.
- Anti-inflammatory medications and/or steroid injections may be orderedto treat pain and swelling.
- Physical therapy may be ordered for strengthening and stretching exercises to the forearm once your symptoms have decreased.
- Pulsed ultrasound may be utilized to increase blood flow and promote healing to the injured tendons.
If conservative treatment options fail to resolve the condition and symptoms persist for 6 -12 months, your surgeon may recommend a surgical procedure to treat tennis elbow called lateral epicondyle release surgery. Your surgeon will decide whether to perform your surgery in the traditional open manner (single large incision) or endoscopically (2 to 3 tiny incisions and the use of an endoscope -narrow lighted tube with a camera). Your surgeon will decide which options are best for you depending on your specific circumstances.
Your surgeon moves aside soft tissue in order to view the extensor tendon and its attachment on the lateral epicondyle. The surgeon then trims the tendon or releases the tendon and then reattaches it to the bone. Any scar tissue present will be removed as well as any bone spurs. After the surgery is completed, the incision(s) are closed by suturing or by tape.
Following surgery, you are referred to physical therapy to improve the range of motion and strength of your joint.
Golfer's Elbow(Medial Epicondylitis)
Golfer's elbow, also called Medial Epicondylitis, is a painful condition occurring from repeated muscle contractions in the forearm that leads to inflammation and microtears in the tendons that attach to the medial epicondyle. The medial epicondyle is the bony prominence that is felt on the inside of the elbow.
Golfer's elbow and Tennis Elbow are similar except that Golfer's elbow occurs on the inside of the elbow and Tennis Elbow occurs on the outside of the elbow. Both conditions are a type of Tendonitis which literally means "inflammation of the tendonitis".
Signs and symptoms
Signs and symptoms of Golfer's Elbow can include the following:
- Elbow pain that appears suddenly or gradually
- Achy pain to the inner side of the elbow during activity
- Elbow stiffness with decreased range of motion
- Pain may radiate to the inner forearm, hand or wrist
- Weakened grip
- Pain worsens with gripping objects
- Pain is exacerbated in the elbow when the wrist is flexed or bent forward toward the forearm
Causes
Golfer's Elbow is usually caused by overuse of the forearm muscles and tendons that control wrist and finger movement but may also be caused by direct trauma such as with a fall, car accident, or work injury.
Golfer's elbow is commonly seen in golfer's, hence the name, especially when poor technique or unsuitable equipment is used when hitting the ball. Other common causes include any activity that requires repetitive motion of the forearm such as: painting, hammering, typing, raking, pitching sports, gardening, shoveling, fencing, and playing golf.
Diagnosis
Golfer's Elbow should be evaluated by an orthopedic specialist for proper diagnosis and treatment.
- Medical History
- Physical Examination
- Your physician may order an x-ray to rule out a fracture or arthritis as the cause of your pain.
- Occasionally, if the diagnosis is unclear, your physician may order further tests to confirm golfer's elbow such as MRI, ultrasonography, and injection test
Conservative Treatment Options
Your physician will recommend conservative treatment options to treat the symptoms associated with Golfer's Elbow. These may include the following:
- Activity Restrictions: Limit use and rest the arm from activities that worsen symptoms
- Orthotics: Splints or braces may be ordered to decrease stress on the injured tissues
- Ice: Ice packs applied to the injury will help diminish swelling and pain. Ice should be applied over a towel to the affected area for 20 minutes four times a day for a couple days. Never place ice directly over the skin
- Medications: Anti-inflammatory medications and/or steroid injections may be ordered to treat the pain and swelling
- Occupational Therapy: OT may be ordered for strengthening and stretching exercises to the forearm once your symptoms have decreased
- Pulsed Ultrasound: A non-invasive treatment used by therapists to break up scar tissue and increase blood flow to the injured tendons to promote healing
- Professional instruction: Consulting with a sports professional to assess and instruct in proper swing technique and appropriate equipment may be recommended to prevent recurrence
Surgery
If conservative treatment options fail to resolve the condition and symptoms persist for 6 -12 months, your surgeon may recommend surgery to treat Golfers Elbow. The goal of surgery to treat Golfers Elbow is to remove the diseased tissue around the inner elbow, improve blood supply to the area to promote healing, and alleviate the patient's symptoms.
Biceps Tendon Rupture
Distal Biceps Rupture
The biceps muscle is located in front of your upper arm. It helps in bending your elbow as well as in rotational movements of your forearm. Also, it helps to maintain stability in the shoulder joint. The biceps muscle has two tendons, one of which attaches it to the bone in the shoulder and the other attaches at the elbow. The biceps tendon at the elbow is called the distal biceps tendon and if there is a tear in this tendon, you will be unable to move your arm from the palm-down to palm-up position. Once the distal biceps tendon is torn, it cannot regrow back to the bone and heal by itself. Permanent weakness during rotatory movements of the forearm may occur if the tendon is not repaired surgically.
Biceps tendon tear can be complete or partial. In partial biceps tendon tear, the tendon does not break up completely. Complete tendon tears will break the tendon into two parts. Tears of the distal biceps tendon are usually complete tears and the muscle gets separated from the bone. They most often result from a sudden injury or lifting a heavy object. Additional risk factors such as advancing age, smoking, and use of corticosteroid medications can also result in increased muscle and tendon weakness.
The most common symptom is a sudden, severe pain in the upper arm or at the elbow. You may feel a "pop" at the elbow when the tendon tears. Other symptoms include swelling, visible bruising, weakness in the elbow, trouble turning your arm from a palm up to a palm down position, and a gap in the front of the elbow caused by absence of the tendon. A bulge may also appear in your arm caused by the recoiled, shortened biceps muscle.
Distal biceps tendon rupture is usually diagnosed based on your symptoms, medical history, and physical examination. During the physical examination, your doctor will look for a gap in the tendon by palpating the front part of your elbow. Your doctor will diagnose a partial tear by asking you to bend your arm and tighten the biceps muscle. You may have pain if there is a partial tear. X-rays may be taken to rule out other conditions causing elbow pain. Using an MRI scan your doctor can know whether tear is partial or complete.
There are several procedures to accomplish reattachment of the distal biceps tendon to the forearm bone. Some techniques require two incisions while in others one incision may be sufficient. In some cases, the tendon is reattached using stitches passed through holes drilled in the bone. Sometimes, a small metal implant may be used to attach the tendon.
Surgical technique
During distal biceps tendon repair, your surgeon makes a small incision over the upper forearm, where the biceps muscle attaches to the radius bone. The torn biceps tendon is brought up through the incision. Then, the radius bone is prepared for tendon reattachment and to promote healing. Two suture anchors will be inserted into the bone. These serve as anchorage for the tendon. The sutures from the suture anchors are passed through the tendon in a particular interlocking manner so as to ensure a strong tendon repair.
After the repair is complete, a hinged elbow brace will be applied with your elbow bent at 90 degrees. The brace will be removed after 6 weeks and it may take up to 6months -1 year to regain full strength.
Biceps Tendon Repair

The biceps muscle is located in front of your upper arm. It helps in bending your elbow as well as in rotational movements of your forearm. Also, it helps to maintain stability in the shoulder joint. The biceps muscle has two tendons, one of which attaches it to the bone in the shoulder and the other attaches at the elbow. The biceps tendon at the elbow is called the distal biceps tendon and if there is a tear in this tendon, you will be unable to move your arm from the palm-down to palm-up position. Once the distal biceps tendon is torn, it cannot regrow back to the bone and heal by itself. Permanent weakness during rotatory movements of the forearm may occur if the tendon is not repaired surgically.
There are several procedures to accomplish reattachment of the distal biceps tendon to the forearm bone. Some techniques require two incisions while in others one incision may be sufficient. In some cases, the tendon is reattached using stitches passed through holes drilled in the bone. Sometimes, a small metal implant may be used to attach the tendon.
Surgical technique
During distal biceps tendon repair, your surgeon makes a small incision over the upper forearm, where the biceps muscle attaches to the radius bone. The torn biceps tendon is brought up through the incision. Then, the radius bone is prepared for tendon reattachment and to promote healing. Two suture anchors will be inserted into the bone. These serve as anchorage for the tendon. The sutures from the suture anchors are passed through the tendon in a particular interlocking manner so as to ensure a strong tendon repair.
After the surgery
After the repair is complete, a hinged elbow brace will be applied with your elbow bent at 90 degrees. The brace will be removed after 6 weeks and it may take up to 6months -1 year to regain full strength.
Risks and Complications
Complications are rare and may include numbness and weakness in the forearm, formation of new bone, limited movement, and re-tearing may occur.
Ulnar Collateral Ligament (UCL) Tear
Introduction
Ulnar collateral ligament (UCL) Reconstruction surgery involves replacing a torn ulnar collateral ligament with a tendon from elsewhere in the body. It is also referred to as Tommy John Surgery.
The UCL, also called medial collateral ligament, is located on the inside of the elbow and connects the ulna bone to the humerus bone. It is one of the main stabilizing ligaments in the elbow especially with overhead activities such as throwing and pitching. When this ligament is injured, it can end a professional athlete's career unless surgery is performed.
Symptoms
The common symptoms associated with a UCL injury are as follows:
- Pain on inner side of the elbow
- Unstable elbow joint
- Numbness in the little finger or ring finger
- Decreased performance in activities such as throwing baseballs or other objects
Causes
Ulnar collateral ligament injury is usually caused by repetitive overhead throwing such as in baseball. The stress of repeated throwing on the elbow causes microscopic tissue tears and inflammation. With continued repetition, eventually the UCL can tear preventing the athlete from throwing with significant speed. If untreated, it can end an athlete's professional career. UCL injury may also be caused by direct trauma such as with a fall, car accident, or work injury. Other causes include any activity that requires repetitive overhead motion of the arm such as tennis, pitching sports, fencing, and painting.
Diagnosis
UCL injury should be evaluated by an orthopedic specialist for proper diagnosis and treatment. Your physician will perform the following:
- Medical history
- Physical examination including a valgus stress test to assess for elbow instability
Other tests such as X-rays and MRI scans may be ordered to confirm the diagnosis.
Treatment
Your physician will recommend conservative treatment options to treat the symptoms associated with UCL injury unless you are a professional or collegiate athlete. In these cases, if the patient wants to continue in their sport, surgical reconstruction is performed.
Conservative treatment options that are commonly recommended for non-athletes include the following:
- Activity restrictions
- Orthotics
- Ice compression
- Medications
- Physical therapy
- Pulsed ultrasound to increase blood flow to the injured ligament and promote healing
- Professional instruction
Procedure
If conservative treatment options fail to resolve the condition and symptoms persist for 6-12 months, your surgeon may recommend ulnar collateral ligament reconstruction surgery. UCL reconstruction surgery repairs the UCL by reconstructing it with a tendon from the patient's own body (autograft) or from a cadaver (allograft). The most frequently used tissue is the palmaris longus tendon in the forearm. The basic steps for UCL reconstruction surgery includes the following:
- The surgery is performed in an operating room under regional or general anesthesia
- Your surgeon will make an incision over the medial epicondyle area
- Care is taken to move muscles, tendons, and nerves out of the way
- The donor tendon is harvested from either the forearm or below the knee
- Your surgeon drills holes into the ulna and humerus bones
- The donor tendon is then inserted through the drilled holes in a figure 8 pattern
- The tendon is attached to the bone surfaces with special sutures
- The incision is closed and covered with sterile dressings
Finally, a splint is applied with the elbow flexed at 90 degrees.
Post-operative care
After surgery, your surgeon will give you guidelines to follow, depending on the type of repair performed and the surgeon's preference. Common post-operative guidelines include:
- Elevate your arm above heart level to reduce swelling
- Wear an immobilizing splint or cast for 1-3 weeks
- Apply ice packs to the surgical area to reduce swelling
- Keep the surgical incision clean and dry. Cover the area with plastic wrap when bathing or showering
- Physical therapy will be ordered for strengthening and stretching exercises after the removal of the splint or cast
- Professional athletes can expect a strenuous strengthening and range of motion rehabilitation program for 6-12 months before returning to their sport
- Eating a healthy diet and not smoking will promote healing
Risks and complications
As with any major surgery there are potential risks involved.
The majority of patients suffer from no complications following UCL Reconstruction surgery, however, complications can occur following elbow surgery and include:
- Infection
- Limited range of motion
- Nerve damage causing numbness, tingling, burning or loss of feeling in the hand and forearm area
- Cubital Tunnel Syndrome
- Elbow instability
Cubital Tunnel Syndrome

Cubital Tunnel Syndrome is a condition characterized by compression of the ulnar nerve in an area of the elbow called the cubital tunnel.
The ulnar nerve travels down the back of the elbow behind the bony bump called the medial epicondyle, and through a passageway called the cubital tunnel. The cubital tunnel is a narrow passageway on the inside of the elbow formed by bone, muscle, and ligaments with the ulnar nerve passing through its center. The roof of the cubital tunnel is covered with a soft tissue called fascia.
When the elbow is bent, the ulnar nerve can stretch and catch on the bony bump. When the ulnar nerve is compressed or entrapped, the nerve can tear and become inflamed leading to a variety of symptoms, called cubital tunnel syndrome.
Signs and Symptoms
In general, signs and symptoms of Cubital Tunnel Syndrome arise gradually, progressing to the point where the patient seeks medical attention. Left untreated, Cubital Tunnel Syndrome can lead to permanent nerve damage in the hand. Commonly reported symptoms associated with Cubital Tunnel Syndrome include:
- Intermittent numbness, tingling, and pain to the little finger, ring finger, and the inside of the hand. These symptoms occur more frequently at night, and with elbow bending or prolonged resting on the elbow.
- Aching pain to the inside of the elbow
- Weakness in hand with diminished grip strength
- Diminished sensation and fine motor control in the hand causing the person to drop objects or have difficulty in handling small objects.
- Muscle wasting in the hand and permanent nerve damage, if left untreated.
Causes
The common causes responsible for cubital tunnel syndrome, include:
- Trauma
- Repetitive motion
- Frequent pressure on the elbow for extended periods due to sitting posture
- Medical Conditions such as bone spurs, ganglion cysts, or tumors in the cubital tunnel leading to pressure and irritation of the ulnar nerve.
- Medical History
- Physical Examination
- Avoid frequent bending of the elbow.
- Avoid pressure to the elbow by not leaning on it. Elbow pads may be worn to decrease pressure when working at a desk.
- Wear a brace or splint at night while sleeping to keep the elbow in a straight position. You can also wrap the arm loosely with a towel and apply tape to hold in place.
- Avoid activities that tend to bring on the symptoms.
- NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) such as ibuprofen or aspirin, may be ordered to reduce swelling.
- Referral to OT (Occupational Therapy) for instruction in strengthening and stretching exercises may be recommended.
- A bulky dressing with a plaster splint is usually applied following surgery for 10-14 days.
- Elevating the arm above heart level and moving the fingers are important to prevent swelling.
- The arm dressing is removed after 10-14 days for removal of the sutures.
- Elbow immobilization for 3 weeks after surgery is usually indicated, longer depending on the repair performed.
- Ice packs are applied to the surgical area to reduce swelling. Ice should be applied over a towel to the affected area for 20 minutes every hour. Keep the surgical incision clean and dry. Cover the area with plastic wrap when bathing or showering.
- Occupational Therapy will be ordered a few weeks after surgery for strengthening and stretching exercises to maximize use of the hand and forearm
- Infection
- Nerve damage causing permanent numbness around the elbow or forearm.
- Elbow instability
- Elbow flexion contracture
- Pain at site of scar
- Symptoms unresolved even after the surgery
Diagnosis
Your physician will perform the following:
Your physician may order X-ray and electro diagnostic tests such as electromyography and nerve conduction studies. These tests can assist your doctor in determining how well the nerve is functioning and locate areas of muscle wasting and nerve compression.
Treatment
Your physician will recommend conservative treatment options initially to treat the symptoms unless muscle wasting or nerve damage is present.
Conservative treatment options may include:
If conservative treatment options fail to resolve the condition or if muscle wasting or severe nerve compression is present, your surgeon may recommend a surgical procedure to treat your condition.
The goal of Cubital Tunnel surgery is to reduce the pressure on the ulnar nerve by providing more space for the nerve to move freely and to increase blood flow to promote healing of the ulnar nerve. There are different surgeries that can be performed to treat your condition, such as:
Medial Epicondylectomy: This surgery involves removing the medial epicondyle, the bony bump on the inside of the elbow, enabling the ulnar nerve to glide smoothly when the elbow is flexed and straightened.
Ulnar Nerve Transposition: This surgery involves creating a new tunnel in front of the medial epicondyle and transposing (moving) the ulnar nerve to the new tunnel.
Your surgeon will decide which options are best for you depending on your specific circumstances.
Post-Operative Care
After surgery, your surgeon will give you guidelines to follow depending on the type of repair performed and the surgeon's preference. Common post-operative guidelines include:
Risks and Complications
The majority of patients suffer no complications following Cubital Tunnel surgery, however, complications can occur following elbow surgery and include:
Elbow Fractures

Three bones, the humerus, radius and ulna, make up the elbow joint. Elbow fractures may occur from trauma, resulting from various reasons; some of them being a fall on an outstretched arm, a direct blow to the elbow, or an abnormal twist to the joint beyond its functional limit. The types of elbow fractures include:
- Radial head and neck fractures: Fractures in the head portion of the radius bone are referred to as radial head and neck fractures.
- Olecranon fractures: These are the most common elbow fractures, occurring at the bony prominence of the ulna.
- Distal humerus fractures: These fractures are common in children and elderly people. Nerves and arteries in the joint may sometimes be injured in these fractures.
Symptoms of an elbow fracture include pain, bruising, stiffness, swelling in and around the elbow, a popping or cracking sound, numbness or weakness in the arm, wrist and hand, and deformity of the elbow bones.
To diagnose an elbow fracture X-rays of the joint are taken. In some cases, a CT scan may be needed to view the details of the joint surface.
The aim of treatment is to maximize early motion and to reduce the risk of stiffness. Nonsurgical treatment options include pain medication, ice application, the use of a splint or a sling to immobilize the elbow during the healing process and physical therapy. Surgery is indicated in displaced and open fractures to realign the bones and stabilize the joint with screws, plates, pins and wires. Strengthening exercises are recommended to improve the range of motion.
Location & Directions
Motion Orthopaedics
633 Emerson Road, Suite 100
Creve Coeur, MO 63141
Tel: 314.991.2107
Fax: 314.991.2108

