

Shoulder
Normal Anatomy of The Shoulder Joint
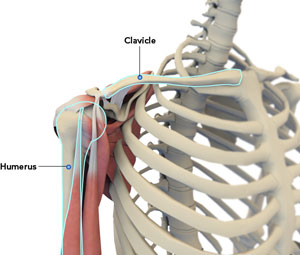
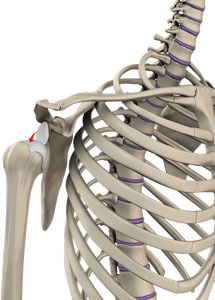
The shoulder is the most flexible joint in the body making it the most susceptible to instability and injury. It is a 'ball-and-socket' joint. A 'ball' at the top of the upper arm bone, humerus, fits neatly into a 'socket', called the glenoid, which is part of the shoulder blade, scapula.
The shoulder joint is made up several bones and soft tissues. It has three bones, the collarbone (clavicle), scapula, and humerus.
Humerus provides attachment to muscles of the upper arm. Scapula is the bone that connects the upper arm bone with the collarbone. It is a flat bone and roughly triangular in shape and provides attachment to the muscles of back and neck.
The clavicle is an S-shaped short bone that connects the shoulder girdle to the body (trunk). It supports the shoulder in a functional position with the axial skeleton so that the arm has maximum range of movement. It also protects major underlying nerves and blood vessels as they pass from the neck to the axilla.
The coracoid process is the extension of the scapula around the shoulder joint at the front portion of the scapula. The acromial process is the extension of scapula around the shoulder joint at the back that forms a roof, acromion.
Glenoid is the smooth shallow depression at the end of scapula that forms the socket of shoulder joint.
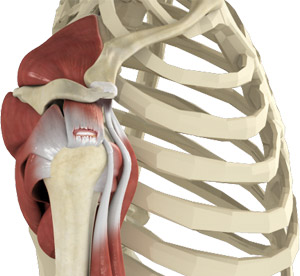
The soft tissues of shoulder joint include:
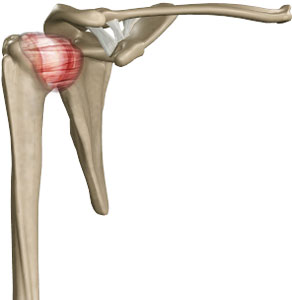
Rotator cuff- A group of 4 tendons make rotator cuff and it holds the head of the humerus in the socket.
Biceps tendon- The biceps tendon is a long cord-like structure which attaches the biceps muscle to the shoulder and helps to stabilize the joint.
Caraco Clavicular Ligament- This ligament connects the clavicle with the corocoid process of the scapula.
Acromio Clavicular Ligament- It connects the clavicle with the acromion process.
Glenoid labrum- The Glenoid labrum is a ring of fibro cartilage surrounding the cavity of the scapula for stabilization of the shoulder joint.
Articular cartilage or the capsule- It is a capsule that surrounds the shoulder joint and helps to keep the ball and socket normally aligned.
Shoulder Arthroscopy
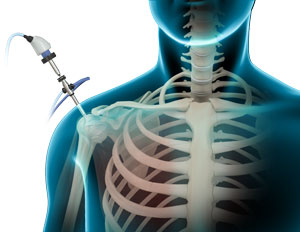
Arthroscopy is a minimally invasive diagnostic and surgical procedure performed for joint problems. Shoulder arthroscopy is performed using a pencil-sized instrument called an Arthroscope. The arthroscope consists of a light system and camera to project images to a computer screen for your surgeon to view the surgical site. Arthroscopy is used to treat disease conditions and injuries involving the bones, cartilage, tendons, ligaments, and muscles of the shoulder joint.
Disease Overview
The shoulder joint is made up of a ball and socket joint, where the head of the humerus (upper arm bone) articulates with the socket of the scapula (shoulder blade) called the glenoid. The two articulating surfaces of the bones are covered with cartilage, which prevents friction between the moving bones enabling smooth movement. Tendons and ligaments around the shoulder joint provide strength and stability to the joint. Injury and disease to the bones or soft tissues of the shoulder joint can make it instable, and lead to pain, inflammation and reduced mobility.
Indications
Shoulder arthroscopy is indicated to treat the following shoulder conditions when conservative treatment such as medication and therapy fails to relieve pain and disability:
- Shoulder Impingement: this occurs when the shoulder blade applies pressure on the underlying soft tissues when the arm is lifted
- Rotator cuff tear
- Frozen shoulder or stiffness of the shoulder joint
- Shoulder Instability this occurs when the head of the upper arm bone slips out of the socket of the shoulder blade's glenoid cavity either due to injury or overuse
- Biceps rupture occurs when the tendons attaching the bicep muscle to the shoulder or elbow tears
- Damaged cartilage or ligaments
- Bone spurs or bony projections
- Arthritis of the collarbone
Procedure
Your surgeon performs shoulder arthroscopy under general or regional anesthesia. You may be positioned lying down on your side with your arm propped up or sitting in a semi-seated position. Sterile fluid is injected into the shoulder joint to expand the surgical area so your surgeon has a clear view of the damage and room to work. A button-sized hole is made in the shoulder and the arthroscope is inserted. Your surgeon can view images captured by the camera in the arthroscope on a large monitor. Surgical instruments are introduced into the joint through separate small holes to remove and repair the damage to the joint. After surgery, the instruments are removed and the incisions are closed with stitches or small sterile bandage strips.
Post-operative Care
After the surgery, the small surgical wounds take a few days to heal and the surgical dressing is replaced by simple Band-Aids. The recovery time depends on the type and extent of problem for which the procedure was performed. Pain medications are prescribed to keep you comfortable. The arm of the affected shoulder is placed in a sling for a short period as recommended by your doctor. Physical therapy is advised to improve shoulder mobility and strength after the surgery.
Advantages
The advantages of arthroscopy compared to open surgery with a large incision include
- Less pain
- Fewer complications
- Shorter hospital stay
- Faster recovery
Risks and complications
Complications of shoulder arthroscopy include infection, bleeding, damage to nearby nerves or blood vessels, or delayed healing after the surgery. In certain cases, stiffness of the shoulder joint may occur after the surgery. It is important to participate actively in your physical therapy to prevent this from occurring.
Rotator Cuff Tear
Rotator cuff is the group of tendons in the shoulder joint providing support and enabling wider range of motion. Major injury to these tendons may result in tear of these tendons and the condition is called as rotator cuff tear. It is one of the most common causes of shoulder pain in middle aged adults and older individuals.
Causes
Rotator cuff tear results from pressure on the rotator cuff from part of the shoulder blade (scapula) as the arm is lifted. It may occur with repeated use of arm for overhead activities, while playing sports or during motor accidents.
Symptoms
Rotator cuff tear causes severe pain, weakness of the arm, and crackling sensation on moving shoulder in certain positions. There may be stiffness, swelling, loss of movements, and tenderness in the front of the shoulder.
Diagnosis
Your surgeon diagnoses Rotator Cuff Tear based on the physical examination, X-rays, and imaging studies, such as MRI. Rotator cuff tear is best viewed on magnetic resonance imaging.
Conservative Treatment Options
- Rest
- Shoulder sling
- Pain medication Injection of a steroid (cortisone) and a local anesthetic in the subacromial space of the affected shoulder to help decrease the inflammation and pain
- Certain Exercises
Surgery
Rotator cuff repair may be performed by open surgery or arthroscopic procedure. In arthroscopy procedure space for rotator cuff tendons will be increased and the cuff tear is repaired using suture anchors. These anchor sutures help in attaching the tendons to the shoulder bone. Following the surgery, you may be advised to practice motion and strengthening exercises.
Shoulder Impingement
Shoulder impingement is the condition of inflammation of the tendons of the shoulder joint. It is one of the most common causes of pain in the adult shoulder. The shoulder is a 'ball-and-socket' joint. A 'ball' at the top of the upper arm bone, humerus, fits neatly into a 'socket', called the glenoid, which is part of the shoulder blade, scapula. Shoulder impingement is also called as swimmer's shoulder, tennis shoulder, or rotator cuff tendinitis.
Causes
Impingement results from pressure on the rotator cuff from part of the shoulder blade (scapula) as the arm is lifted. It is more likely to occur in young and middle aged people who engage in physical activities that require repeated overhead arm movements. The pain may be due to a "bursitis" or inflammation of the bursa overlying the rotator cuff or a "tendonitis" of the cuff itself. In some circumstances, a partial tear of the rotator cuff may cause impingement pain.
Symptoms
Individuals with shoulder impingement may experience severe pain at rest and during activities, weakness of the arm and difficulty in raising the hand overhead.
Diagnosis
Diagnosis involves physical examination by the doctor where in the doctor checks for the possible range of movements with the affected shoulder. X-rays and MRI scans may be ordered to see the injury and inflammation.
Conservative Treatment Options
Shoulder impingement can be treated with rest, ice packs, anti-inflammatory drugs, and avoiding the activities involving the shoulder. Physical therapy may be advised to strengthen the muscles and steroid injections may be given if pain persists.
Surgery
Arthroscopic surgery is recommended if the rotator cuff tendons are torn and to remove the bony spurs.
Frozen Shoulder(Adhesive Capsulitis)
Frozen shoulder, also called adhesive capsulitis is a condition characterized by pain and loss of motion in shoulder joint. It is more common in older adults aged between 40 and 60 years and is more common in women than men.
Causes
Frozen shoulder is caused by inflammation of the ligaments holding the shoulder bones to each other. The shoulder capsule becomes thick, tight, and the stiff bands of tissue called adhesions may develop. Individuals with shoulder injury, shoulder surgeries, shoulder immobilized for longer period of time, other disease conditions such as diabetes, hypothyroidism, hyperthyroidism, Parkinson's disease and cardiac diseases are at risk of developing frozen shoulder.
Symptoms
Frozen shoulder may cause pain and stiffness and limit the movements of shoulder.
Diagnosis
Frozen shoulder condition can be diagnosed by the presenting symptoms and radiological diagnostic procedures such as X-rays or MRI scans.Â
Conservative Treatment
Conservative Treatment options include:
- Non-steroidal anti-inflammatory drugs and steroid injections for pain
- Physical therapy to improve your range of motion
- Sometimes heat may be applied to reduce pain
Surgery
Your surgeon may recommend Shoulder arthroscopy when the conservative treatment does not work. During surgery, the scar tissue will be removed and tight ligaments, if any, will be dissected. Following surgery physical therapy will be advised to bring full range of motion and strengthen the muscles.
Adhesive Capsulitis
Injections for Frozen Shoulder
Frozen shoulder, also called adhesive capsulitis is a condition characterized by pain and loss of motion in shoulder joint. It commonly affects the left shoulder than right and occurs more often in women than men. The exact cause of frozen shoulder is not known. It is most commonly associated with diabetes and a few other endocrine diseases. The main symptoms include pain, stiffness, and decreased motion of the shoulder.
Frozen shoulder is a self-limiting disease and symptoms usually subside after a year. Treatment is aimed at pain control and restoration of motion.
The treatment of frozen shoulder requires a combination of non-steroidal anti-inflammatory medications, steroid injections, and physical therapy.
Cortisone injections: Cortisone injections are given directly into, or near to the shoulder joint. It reduces the inflammation within the frozen shoulder joint. Cortisone is a type of corticosteroid released by the adrenal gland in response to stress.
Cortisone is a potent anti-inflammatory medicine that can reduce inflammation, but is not pain reliever. Cortisone injections typically result in pain relief within a few days, which is because the inflammation diminishes. The effects may last for several weeks.
The most common side effect is a "cortisone flare". This is a condition where the injected cortisone crystallizes and causes a brief period of severe pain, that usually only lasts for a day or two. This is treated by application of ice to the injected area. Other side effects include whitening of the skin at the injection site, infection, a transient elevation in their blood sugar in patients with diabetes.
Arthroscopic capsular releases/manipulation
Arthroscopic capsular release and manipulation under anesthesia (MUA) are the surgical procedures performed to treat the frozen shoulder. Frozen shoulder, also called adhesive capsulitis is a condition characterized by pain and loss of motion in shoulder joint.
This procedure is extremely useful in cases of frozen shoulder that do not respond to therapy and rehabilitation. The aim of the surgery is to decrease pain, reduce the recovery time and help to gain full range of movement.
A manipulation under anesthesia (MUA) is most commonly indicated in patients with simple frozen shoulder. This procedure is performed with the patient sedated under anesthesia. Your surgeon moves the shoulder through a range of motion which causes the capsule and scar tissue to stretch or tear. Thus, the tight capsule is released allowing increased range of motion. The procedure involves freeing the shoulder by manipulation and does not involve any incisions.
Arthroscopic capsular release is a keyhole surgery that involves the release of the tight, constricted capsule. During the procedure 2 to 3 holes are made in the shoulder. The thickened, swollen abnormal capsule tissue is cut and removed using a special radiofrequency thermal probe. It is an effective treatment for most people with stiff shoulder after injury, trauma, or fracture, and diabetes.
Following capsular release, immediate rehabilitation is necessary to prevent the recurrence of frozen shoulder. The aim of the rehabilitation is to reduce pain and to restore full range of motion.
- Pain medications are recommended to control pain
- Following these procedures regular exercises need to be done in order to achieve full range of motion
- If you feel comfortable and have good range of movement, you can begin driving 1 week after your surgery
- Returning to work depends on the nature of your work. If you are in a sedentary job you may be able to return as early as 1 week after surgery but if your job requires heavy lifting or using your arm at shoulder height, it may take longer time to return to your work
- Full range of motion is achieved at 4 - 6 weeks
An appointment with the physiotherapist will be arranged in the first week following your surgery. The amount of exercises you require will depend on your progress.
Shoulder Instability & Dislocation
Shoulder instability is a chronic condition that causes frequent dislocations of the shoulder joint.
Causes
A dislocation occurs when the end of the humerus (the ball portion) partially or completely dislocates from the glenoid (the socket portion) of the shoulder. A partial dislocation is referred to as a subluxation whereas a complete separation is referred to as a dislocation.
Risk Factors
The risk factors that increase the chances of developing shoulder instability include:
- Injury or trauma to the shoulder
- Falling on an outstretched hand
- Repetitive overhead sports such as baseball, swimming, volleyball, or weightlifting
- Loose shoulder ligaments or an enlarged capsule
Symptoms
The common symptoms of shoulder instability include pain with certain movements of the shoulder; popping or grinding sound may be heard or felt, swelling and bruising of the shoulder may be seen immediately following subluxation or dislocation. Visible deformity and loss of function of the shoulder occurs after subluxation or sensation changes such as numbness or even partial paralysis can occur below the dislocation as a result of pressure on nerves and blood vessels.
Conservative Treatment
The goal of conservative treatment for shoulder instability is to restore stability, strength, and full range of motion. Conservative treatment measures may include the following:
- Closed Reduction: Following a dislocation, your surgeon can often manipulate the shoulder joint, usually under anesthesia, realigning it into proper position. Surgery may be necessary to restore normal function depending on your situation
- Medications: Over the counter pain medications and NSAID's can help reduce the pain and swelling. Steroidal injections may also be administered to decrease swelling
- Rest: Rest the injured shoulder and avoid activities that require overhead motion. A sling may be worn for 2 weeks to facilitate healing
- Ice: Ice packs should be applied to the affected area for 20 minutes every hour
Surgery
When the conservative treatment options fail to relieve shoulder instability, your surgeon may recommend shoulder stabilization surgery. Shoulder stabilization surgery is done to improve stability and function to the shoulder joint and prevent recurrent dislocations. It can be performed arthroscopically, depending on your particular situation, with much smaller incisions. Arthroscopy is a surgical procedure in which an arthroscope, a small flexible tube with a light and video camera at the end, is inserted into a joint to evaluate and treat of the condition. The benefits of arthroscopy compared to the alternative, open shoulder surgery are smaller incisions, minimal soft tissue trauma, less pain leading to faster recovery.
Labral Tears
The shoulder joint is a "ball and socket" joint that enables the smooth gliding and thereby the movements of arms. However, it is inherently unstable because of the shallow socket. A soft rim of cartilage, the labrum lines the socket and deepens it so that it accommodates the head of the upper arm bone better.
Traumatic injury to the shoulder or overuse of shoulder (throwing, weightlifting) may cause labral tear. In addition, ageing may weaken the labrum leading to injury. Shoulder labral tear injury may cause symptoms such as pain, catching or locking sensation, decreased range of motion and joint instability.
Your doctor may start with conservative approaches such as prescribing anti-inflammatory medications and advice rest to relieve symptoms until diagnostic scans are done. Rehabilitation exercises may be recommended to strengthen rotator cuff muscles. If the symptoms do not resolve with these conservative measures, your doctor may recommend arthroscopic surgery.
During arthroscopic surgery, your surgeon examines the labrum and the biceps tendon. If the damage is confined to the labrum without involving the tendon, then the torn flap of the labrum will be removed. In cases where the tendon is also involved or if there is detachment of the tendon, absorbable wires or sutures will be used to repair and reattach the tendon. After the surgery, you will be given a shoulder sling to wear for 3-4 weeks. You will be advised motion and flexibility exercises after the sling is removed. These exercises increase the range of motion and flexibility of shoulder joint.
SLAP Tears
The shoulder joint is a ball and socket joint. A 'ball' at the top of the upper arm bone (the humerus) fits neatly into a 'socket', called the glenoid, which is part of the shoulder blade (scapula). The term SLAP (superior -labrum anterior-posterior) lesion refers to an injury of the superior labrum of the shoulder. The labrum is a ring of fibrous cartilage surrounding the glenoid for stabilization of the shoulder joint. The biceps tendon attaches inside the shoulder joint at the superior labrum of the shoulder joint. The biceps tendon is a long cord-like structure which attaches the biceps muscle to the shoulder and helps to stabilize the joint.
The most common causes include falling on an outstretched arm, repetitive overhead actions such as throwing, and lifting a heavy object. Overhead and contact sports may put you at a greater risk of developing SLAP lesions.
The most common symptom is pain at the top of the shoulder joint. In addition, catching sensation and pain most often with activities such as throwing may also occur.
Diagnosis is made based on the symptoms and physical examination. A regular MRI scan may not show up a SLAP tear and therefore an MRI with a contrast dye injected into the shoulder, is ordered. The contrast dye helps to highlight SLAP tears.
Your doctor may recommend anti- inflammatory medications to control pain. In athletes who want to continue their sports, arthroscopic surgery of the shoulder may be recommended. Depending on the severity of the lesion, SLAP lesions may simply require debridement or some may need to be repaired. Â A SLAP repair can be done using arthroscopic techniques that require only two or three small incisions.
Regular exercises that make the shoulder muscles strong should be done. Adequate warm-up exercises before activities and avoiding high contact sports can help prevent injuries that cause instability.
Pec Rupture
The pectoralis muscle is a large muscle that is located in front of your chest and helps to move your shoulder forwards and across your chest. The pectoralis muscle is divided into the pectoralis major and the pectoralis minor. The pectoralis major muscle is the larger muscle and helps to push the arms in front of the body.
The pectoralis major muscle or its tendon that gets attached to the arm bone (the humerus) can rupture. This is known as a "pec rupture," or a pectoralis major muscle rupture. It is quite rare and occurs only in men between the age of 20 and 50 years. Pectoralis muscle rupture may lead to partial or complete tear of the muscle. Partial ruptures are less common and complete rupture occurs when the tendinous attachment of the muscle to the bone tears.
Torn pectoral muscles are most often caused by forceful activities such as weightlifting, especially during a bench press exercise. The condition might also result from sports such as football, wrestling, rugby, and other traumatic accidents or injuries. These injuries are more likely to occur in patients who use steroid medication.
When the pectoralis muscle ruptures, you will have sudden severe pain and a tearing sensation in the chest. You may also have pain in the upper arm, weakness, bruising, and a dimpling, or pocket formation above the arm pit.
Initial treatment includes application of ice and immobilization of the shoulder, arm and chest. Surgery is often required for complete tears of the pectoralis muscle tendon. Surgery is usually not considered for partial tears, tears within the muscle, or in elderly and low-demand patients. The torn tendon is repaired in the early period following the injury to minimize muscle atrophy and scarring. Patients who undergo surgical repair have a good chance of returning to high-level sports and activities. During the repair, large sutures are placed in the torn tendon and then these sutures are secured to the arm bone with either holes in the bone or anchors inserted in the bone.
Pectoralis muscle rupture can be prevented by following certain instructions on proper bench press technique. For proper bench press technique, it is important to limit the distance to which the bar is lowered, and also narrowing the grip of the hands to the bar.
Clavicle Fractures
Clavicle fracture, also called broken collarbone is a very common sports injury seen in people who are involved in contact sports such as football and martial arts as well as impact sports such as motor racing. A direct blow over the shoulder that may occur during a fall on an outstretched arm or a motor vehicle accident may cause the clavicle bone to break. Broken clavicle may cause difficulty in lifting your arm because of pain, swelling and bruising over the bone.
Broken clavicle bone, usually heals without surgery, but if the bone ends have shifted out of place (displaced) surgery will be recommended. Surgery is performed to align the bone ends and hold them stable during healing. This improves the shoulder strength. Surgery for the fixation of clavicle fractures may be considered in the following circumstances:
- Multiple fractures
- Compound (open) fractures
- Fracture associated with nerve or blood vessel damage and scapula fracture
- Overlapping of the broken ends of bone (shortened clavicle)
Plates and Screws fixation
During this surgical procedure, your surgeon will reposition the broken bone ends into normal position and then uses special screws or metal plates to hold the bone fragments in place. These plates and screws are usually left in the bone. If they cause any irritation, they can be removed after fracture healing is complete.
Pins
Placement of pins may also be considered to hold the fracture in position and the incision required is also smaller. They often cause irritation in the skin at the site of insertion and have to be removed once the fracture heals.
Complications
Patients with diabetes, the elderly individuals and people who make use of tobacco products are at a greater risk of developing complications both during and after the surgery. In addition to the risks that occur with any major surgery, certain specific risks of clavicle fracture surgery include difficulty in bone healing, lung injury and irritation caused by hardware.
Percutaneous elastic intramedullary nailing of the clavicle is a newer and less invasive procedure with lesser complications. It is considered as a safe method for fixation of displaced clavicle fractures in adolescents and athletes as it allows rapid healing and faster return to sports. The procedure is performed under fluoroscopic guidance. It involves a small 1 cm skin incision near the sternoclavicular joint, and then a hole is drilled in the anterior cortex after whichan elastic nail is inserted into the medullary canal of the clavicle. Then the nail is passed on to reach the fracture site. A second operation to remove the nail will be performed after 2-3 months.
Shoulder Arthritis
Glenohumeral DJD and Shoulder Replacement
Glenohumeral degenerative joint disease (GDJD), also known as osteoarthritis of the shoulder, is a condition characterized by degeneration or wearing away of the protective cartilage that covers the ends of your bones (articular cartilage). As a result of degeneration of the articular cartilage the ends of the two bones rub together and form bony growths (osteophytes).
The shoulder is a 'ball-and-socket' joint. The shoulder joint is also called as glenohumeral joint, the joint formed by gelnoid and humerus bones. The shoulder joint is formed when a 'ball' at the top of the upper arm bone, humerus, fits neatly into a 'socket', the glenoid, which is part of the shoulder blade.
Glenohumeral DJD is most often seen in people over 50 years. It can also develop after an injury or trauma to the shoulder. The condition may also be hereditary.
A person with glenohumeral DJD is likely to have tenderness and shoulder pain that aggravates during activity. Swelling of the joint may also be seen. You may hear a clicking or creaking sound as you move your shoulder.
To diagnose glenohumeral DJD, your doctor will take a medical history and performs a physical examination of your shoulder. X-rays of an arthritic shoulder may be useful to see osteophytes and loss of joint space.
Treatment for glenohumeral DJD includes both nonsurgical treatment and surgical treatment. Non-surgical treatment includes use of anti-inflammatory medications, applying ice, moist heat to joint, performing range-of-motion exercises and physical therapy, corticosteroid injections, and dietary supplements of glucosamine and chondroitin.
Surgery may be indicated if nonsurgical treatments are not effective. Glenohumeral DJD can be surgically treated with two forms of replacement, hemiarthroplasty and total shoulder arthroplasty. In total shoulder arthroplasty, the entire shoulder joint is replaced with an artificial joint where as in hemiarthroplasty only the head of the upper arm bone is replaced.
Shoulder Replacement
Shoulder joint replacement is a surgical procedure performed to replace the damaged shoulder joint with the artificial joint parts. Shoulder joint replacement is usually performed when the joint is severely damaged by osteoarthritis, rheumatoid arthritis, post-traumatic arthritis, rotator cuff tear arthropathy, avascular necrosis, and failed former shoulder replacement surgery.
During the surgery, an incision is made over the affected shoulder to expose the shoulder joint. The humerus is separated from the glenoid socket of the scapula. The arthritic part of the humeral head and the socket is removed and prepared so as to take the artificial components. The glenoid component is then pressed into the socket, and the humeral component is cemented into the upper arm bone. The humeral head component made of metal is then placed on the humeral stem. The artificial components are fixed in place. The joint capsule is stitched together. The muscle and tendons are then repaired and the skin is closed.
Possible risks and complications specific to shoulder joint replacement surgery include:
- Infection around an implanted joint
- Dislocation or instability of an implanted joint
- Fracture of the humerus or scapula
- Damage to nerves or blood vessels
- Blood clots (deep vein thrombosis)
- Wound irritation
- Arm length discrepancies
- Wearing of the joints
- Scar formation
AC Joint Arthrosis and Reconstruction
Acromioclavicular (AC) joint arthrosis or osteoarthritis of the acromioclavicular joint is a condition that develops when the cartilage cushioning the AC joint in the shoulder begins to wear out. The shoulder is a 'ball-and-socket' joint. A 'ball' at the top of the upper arm bone, humerus, fits neatly into a 'socket', the glenoid, which is part of the shoulder blade, scapula. The shoulder joint is made up of three bones, the collarbone (clavicle), scapula (shoulder bone), and humerus (arm bone). The AC joint is located where the clavicle meets the end of the shoulder blade, acromion.
The AC joint osteoarthritis occurs as a result of repeated movements of the arm and overhead activities. People who lift heavy weights overhead such as weightlifters and those involved in overhead sports such as basketball are at increased risk for developing osteoarthritis of the AC joint. Another common cause is a previous injury to the AC joint causing AC joint separation.
Osteoarthritis in the AC joint may cause pain and tenderness in front of the shoulder. Moving the affected arm across your chest may compress the AC joint and worsen the pain. Pain also radiates to the shoulder, front of the chest, and the neck. In patients who had previous shoulder injury, bumps appear around the AC joint. You can hear a snap or click when you move your affected shoulder.
Diagnose of AC joint osteoarthritis will be made by collecting medical history and physical examination. During physical examination, your doctor will look for tenderness over the AC joint and pain with compression of the AC joint. To confirm the diagnosis a local anesthesia may be injected into the joint to temporarily reduce the pain. X-rays of the AC joint will be taken to reveal bone spurs around the joint and narrowing of the joint space.
Treatment for AC joint osteoarthritis includes both nonsurgical treatment and surgical treatment. Non-surgical treatment includes rest, use of nonsteroidal anti-inflammatory medications, physical therapy, and injections of corticosteroids. Surgery may be indicated if nonsurgical treatments are not effective. Resection arthroplasty is the surgery of choice for AC joint osteoarthritis. During this surgery, your doctor removes about half-inch of the clavicle bone at the end where it meets the scapula. As the process of healing, scar tissue will fill the space created by removal of a piece of clavicle bone. The scar tissue allows normal movement of the AC joint and avoids rubbing of bone ends. The surgery may be performed using minimally invasive technique or using arthroscope.
AC Joint Reconstruction
Of late, research has been focused on improving surgical techniques used to reconstruct the severely separated AC joint. The novel reconstruction technique that has been designed to reconstruct the AC joint in an anatomic manner is known as anatomic reconstruction. Anatomic reconstruction of the AC joint ensures static and safe fixation and stable joint functions. Nevertheless, a functional reconstruction is attempted through reconstruction of the ligaments. This technique is done through an arthroscopically assisted procedure. A small open incision will be made to place the graft.
This surgery involves replacement of the torn CC ligaments by utilizing allograft tissue. The graft tissue is placed at the precise location where the ligaments have torn and fixed using bio-compatible screws. The new ligaments gradually heal and help restore the normal anatomy of the shoulder.
Postoperative rehabilitation includes use of shoulder sling for 6 weeks followed by which physical therapy exercises should be done for 3 months. This helps restore movements and improve strength. You may return to sports only after 5-6 months after surgery.
AC joint Arthritis
Acromioclavicular (AC) joint arthrosis or osteoarthritis of the acromioclavicular joint is a condition that develops when the cartilage cushioning the AC joint in the shoulder begins to wear out. The shoulder is a 'ball-and-socket' joint. A 'ball' at the top of the upper arm bone, humerus, fits neatly into a 'socket', the glenoid, which is part of the shoulder blade, scapula. The shoulder joint is made up of three bones, the collarbone (clavicle), scapula (shoulder bone), and humerus (arm bone). The AC joint is located where the clavicle meets the end of the shoulder blade, acromion.
The AC joint osteoarthritis occurs as a result of repeated movements of the arm and overhead activities. People who lift heavy weights overhead such as weightlifters and those involved in overhead sports such as basketball are at increased risk for developing osteoarthritis of the AC joint. Another common cause is a previous injury to the AC joint causing AC joint separation.
Osteoarthritis in the AC joint may cause pain and tenderness in front of the shoulder. Moving the affected arm across your chest may compress the AC joint and worsen the pain. Pain also radiates to the shoulder, front of the chest, and the neck. In patients who had previous shoulder injury, bumps appear around the AC joint. You can hear a snap or click when you move your affected shoulder.
Diagnose of AC joint osteoarthritis will be made by collecting medical history and physical examination. During physical examination, your doctor will look for tenderness over the AC joint and pain with compression of the AC joint. To confirm the diagnosis a local anesthesia may be injected into the joint to temporarily reduce the pain. X-rays of the AC joint will be taken to reveal bone spurs around the joint and narrowing of the joint space.
Treatment for AC joint osteoarthritis includes both nonsurgical treatment and surgical treatment. Non-surgical treatment includes rest, use of nonsteroidal anti-inflammatory medications, physical therapy, and injections of corticosteroids. Surgery may be indicated if nonsurgical treatments are not effective. Resection arthroplasty is the surgery of choice for AC joint osteoarthritis. During this surgery, your doctor removes about half-inch of the clavicle bone at the end where it meets the scapula. As the process of healing, scar tissue will fill the space created by removal of a piece of clavicle bone. The scar tissue allows normal movement of the AC joint and avoids rubbing of bone ends. The surgery may be performed using minimally invasive technique or using arthroscope.
AC Joint Reconstruction
Of late, research has been focused on improving surgical techniques used to reconstruct the severely separated AC joint. The novel reconstruction technique that has been designed to reconstruct the AC joint in an anatomic manner is known as anatomic reconstruction. Anatomic reconstruction of the AC joint ensures static and safe fixation and stable joint functions. Nevertheless, a functional reconstruction is attempted through reconstruction of the ligaments. This technique is done through an arthroscopically assisted procedure. A small open incision will be made to place the graft.
This surgery involves replacement of the torn CC ligaments by utilizing allograft tissue. The graft tissue is placed at the precise location where the ligaments have torn and fixed using bio-compatible screws. The new ligaments gradually heal and help restore the normal anatomy of the shoulder.
Postoperative rehabilitation includes use of shoulder sling for 6 weeks followed by which physical therapy exercises should be done for 3 months. This helps restore movements and improve strength. You may return to sports only after 5-6 months after surgery.
AC Separation
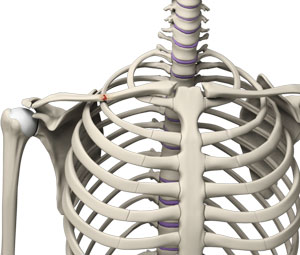
The acromioclavicular joint (AC joint) is one of the 3 joints in the shoulder and connects the clavicle (collar bone) to the scapula (shoulder blade). The AC joint is held with 4 main ligaments, the superior (above the joint) and inferior (below the joint) ligaments, the coracoclavicular ligaments, and the coracoacromial ligament.
Coracoclavicular ligaments are the ligaments that connect the coracoids process (bony prominence on the scapula) and the clavicle. Coracoacromial ligament connects the acromion to the coracoid process. Injury to AC joint causes separation and the tear of ligaments. More severe cases require AC joint reconstruction surgery to stabilize the joint which involves replacement of torn ligaments and stabilizing the reconstruction.
Modified Weaver-Dunn Technique
The original Weaver-Dunn procedure involves removal of a portion of clavicle bone at its lateral end, separation of coracoacromial ligament from acromion, preparation of coracoacromial ligament and reattachment of the ligament to clavicle bone. The modified Weaver-Dunn technique involves additional stabilization of the transferred ligament using screws or suture around the coracoids & clavicle.
During the procedure, surgeon expose AC joint by an incision from top-front of the shoulder extending down over the coracoids process. The lateral end of the clavicle is cut in oblique angle and the coracoacromial ligament is detached along with a piece of bone from acromion. Surgeon drills holes in clavicle bone to fix the detached coracoacromial ligament and also drills the inner core of clavicle. Then the new ligament is pulled in to the cavity and is secured using the suture cords. Furthermore, a suture cord is passed around the base of coracoids and clavicle to stabilize the reconstruction. Following reconstruction and stabilization the surrounding muscles are repaired and incisions are closed.
Postoperative rehabilitation includes use of shoulder sling for 6 weeks followed by physical therapy exercises. This helps restore movements and improve strength. All movements and activities above the shoulder level must be avoided for first 12 weeks following surgery.
The most common complications of surgery include infection, nerve and blood vessel injuries, continued pain or stiffness, fracture, unsuccessful surgery, ligaments re-tear, and revision surgery.

